We’re back for part two! If you haven’t read the first part of this series check it out here! Part one focused on the language we use with our children to discuss food, primarily focusing on what we can add in/highlight vs omit. Part two will focus on supporting parents’ with weight and health conversations.
As mentioned in part one, we cannot control every aspect of what our kids see and hear (even if we want to) but we can help them to process and make some sense of it all!
What to know and say about weight
As a health professional, weight is often discussed in regards to a person’s health (more to come on this). For children and teens, it can be a marker of their growth and development (more on this as well). I think it gets confusing when most of the current messaging is promoting weight loss for health and at the same time feels like pretty black and white thinking about bodies: thin = better. This messaging is often meant to be geared towards adults but basically every other ad on TV and social media is marketing weight loss, so it is no surprise that our kids may have thoughts and questions about the connection between weight and health.
For younger children who are not yet on social media or tuning into weight loss commercials, one of the first places your child may see and have conversations around their weight will likely be at medical appointments. Every time a child visits their pediatricians office they will likely have a weight taken by a nurse and then taken back to a room to meet with their provider. I am not a pediatrician so I cannot speak for how each provider approaches the entirety of these appointments, but from my experience as a clinician and a mom, they will often address weight trends and may show you, and your child, the actual growth curves. Providers may then ask questions and give recommendations about nutrition, exercise and screen time.
In preparation for these appointments, it may be helpful to prep your child with what to expect. “When we get there, a nurse will measure how much you’ve grown in a few different ways, like stepping onto a scale and measuring how tall you are, and then we will meet with your doctor to talk about how this past year has been going. How does that sound? Is there anything you want to make sure we talk about or anything you’re feeling nervous about?” You may be able to ask to speak to their provider separately to avoid discussing specific numbers/trends if that feels uncomfortable for you and/or your child.
What about when working with a Registered Dietitian (RD)? We also look at growth curves/trends and work closely with pediatricians to collaborate on recommendations. We will ask about weight and growth history in our initial assessment but we only make this a priority of conversation during sessions if the child/teen is coming to us for support in that area, other providers have shared growth concerns or we hear concerning behaviors around nutrition, body and/or exercise. For some clients, depending on their age and reason for visit, we will request obtaining a blind weight in the office. This is done by turning around backwards on the scale so that the number is only seen by the RD. More often than not, a child is seeing other providers who are taking their weight so we will not take another one in session. In order for us to best support a kiddo who is growing and developing rapidly, we do need to have awareness of growth trends so weight is an important piece of the puzzle but it is not the only piece we focus on. Lastly, we do not expect someone to weigh themselves at home. I have had many clients, of all ages, assume I want them stepping on the scale at home but I certainly do not. We spend time setting other very important goals to focus on other than weight!
Some background on normal weight change
I think it’s incredibly important for parents and children to know what appropriate growth and weight expectations are. When looking at a growth chart, we are looking at where the child has been trending for most of their life and if there any major jumps out of their “normal” curves. Normal for one kid is NOT the same as another. A child who has been tracking in the 95th percentile for height and weight will not have the same growth trends as a child who has followed the 25th percentile for most of their life. There are points in a child’s life where we would expect to see them step out of their normal curve, like growth spurts, especially during puberty and I cannot emphasize enough how normal this is. Rebecca Peebles MD, FAAP who is a well-known pediatrician and serves as the Vice President of Adolescent Medicine at Monte Nido, shares on average, adolescents gain about 40lbs during peak development which is a roughly 2 year period after puberty begins. Please read that again. This weight gain includes much more than simply body fat. For example, this is where most of the skeletal/bone density accrual takes place. The American Academy of Pediatrics states, “Adolescence is of utmost importance with regard to long term bone health because fully half of the adult bone calcium is accreted during these years”.
The reason I find it so important for parents and children to know what’s going on behind the scenes is to have a clear understanding that bodies are supposed to change. Even when height growth stops, bodies are still changing. This can drastically change how we view and discuss weight. When we know more we can ask more. If you or one of your child’s providers notice growth or behavior changes that feel abnormal, you can start to explore more.
For example, if they have not hit an expected growth spurt or puberty yet, consider if you’ve noticed anything different about your child’s mood, sleep, appetite, or desire to be involved (or not) in cooking/shopping/food preparation? You could ask the following:
“Dad and I noticed you’re plating less than normal and going right to your room after dinner. How have you been feeling lately?”
“I noticed that you’re not having an afternoon snack before practice anymore. How has your appetite been?”
“I’m hearing you share a lot of ideas of what you do and do not want for lunch lately. Tell me more about why you’d like things to be different?”
“I’ve noticed you’ve been really tired when you get home. How have you been sleeping?”
Also consider their activity level. Sometimes as a kiddo goes in and out of a sports season or they go from school to a club sport (or are participating in both at the same time!), their energy output will change and they may have a major energy gap between what they’re exerting and what they’re consuming. Growing/developing + being an athlete requires an incredible amount of nutrition. Underfueling can be unintentional (we don’t know what we don’t know) and other times there is more underneath the surface (i.e desire for weight loss). Working with a RD specialized in pediatrics, disordered eating and/or sports nutrition can be really helpful to navigate all of this.
What if we hear our child make comments about disliking their body?
“I need to lose weight.”
“I’m fat. I hate my body.”
This is heart breaking. I love to remind everyone that we have a lot of different emotions, all meant to be felt, but fat is not an emotion. They are likely having some degree of body dissatisfaction that should be explored further and we want to figure out how to hold space for that. If you hear your child make a comment similar to these, first pause and check in with what automatic response you want to say. Sometimes we go immediately into fix-it mode because it can be so difficult to hear their pain and we want to take it away. “No you are not! You are beautiful and perfect”. This may actually invalidate what they are feeling at that moment and put a focus on the idea that having body fat is a bad thing.
There is an amazing resource from Kids Eat in Color RD, Jennifer Abderson where she shares different responses. See below
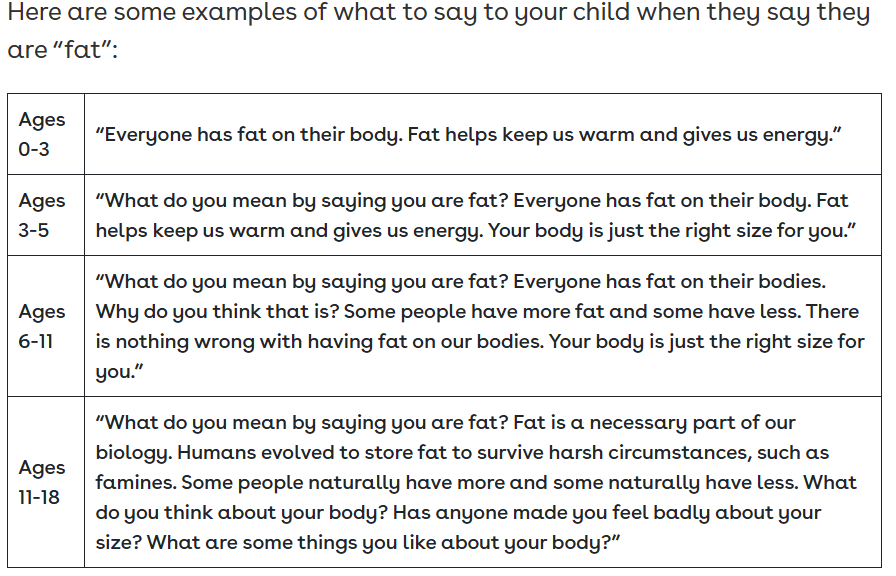
What I would add to this is, for all ages, explore more. Ask how their day went, what conversations they may have had or things they heard at school/with friends. If you think about this experience as your own, it may shed light on what you may want to hear and then what your kid needs to hear. It doesn’t always feel warm and fuzzy when someone says “That’s not true!” or tries to find the bright side right away. Sometimes we want someone to sit in the hard for a second and go “That sounds like a really hard thought to hold onto. You’re really brave for sharing it with me. Tell me more.” Depending on their age you could also say, “It sounds like you are feeling really down about your body. What would better describe how you’re feeling right now besides ‘fat’?” I would also recommend connecting your child with a mental health provider who has experience in disordered eating and body image for additional support
Lastly, health is more than weight
Weight is one part of the health puzzle but it certainly is not the only one. Ultimately, because of the incredible importance of focusing on growth and development for children and teens, I do not recommend pursuing weight loss. We all have a genetic blueprint that guides our appropriate growth trajectories. Weight is not as controllable as it may appear and it’s important for our kids to know that their body isn’t wrong for changing and growing. It’s an issue if it’s not. Instead, we can focus on what actually makes us healthy. You could explore the following with your kiddo and pick an area to focus on:
How is your sleep? 8-12 hours is recommended for most adolescents/teens.
How are your relationships/friendships? Spending time with family and friends is incredibly important for our health!
How do we engage in movement? Movement is a key component of our health AND we want to be mindful of how much we are moving and ensure we also rest, recover and eat enough.
What is our mood and energy like? Not eating or sleeping enough can make us incredibly irritable.
How stressed do we feel? Gauging overall stress from school, home, sports, friendships etc. can help to guide where to add in some self-care.
How is nutrition? Of course as an RD I care so much about nutrition. Are they eating 3 meals + snacks? Are they eating all 5 food groups (protein, carbohydrates, fats, dairy, fruits and vegetables)? Are they able to eat flexibly at parties/holidays?
We want to do things that make our bodies feel good! If pursuing a behavior change leads to someone having lower energy, poor sleep, higher stress, growth concerns or a nutrient imbalance (i.e. iron deficiency) that is not actually in pursuit of health.
Takeaways
It’s a really hard, yet important time to hold space for hard conversations. Knowing what appropriate growth and weight change is becomes crucial for how we have these discussions. When someone is unhappy in their body, their stress and anxiety is palpable. Naming that with our children can be a really helpful connection point and then find ways to collaborate on how to best support them moving forward:
- Discuss what to expect from medical appointments
- Openly discuss that bodies are supposed to change
- Talk with your child’s pediatrician and dietitian about any concern you have with growth or behaviors you are seeing at home
- Focus on what we can add in vs take away
- There is WAY more to health than weight!
Resources:
Anderson, J. (2025, July 8). Child health & weight toolkit for parents. Kids Eat in Color. https://kidseatincolor.com/parent-toolkit/
Anderson, J. (2025b, August 21). How to talk to kids about weight (a guide for parents). Kids Eat in Color. https://kidseatincolor.com/how-to-talk-to-kids-about-weight-and-health/
Crosbie, C., & Sterling, W. (2019). How to nourish your child through an eating disorder. A simple, plate-by-plate approach to rebuilding a healthy relationship with food. Blackstone Publishing.
Peebles, R., Grubiak , K., & Muhlheim, L. (2025, September). Updated Training on Weight-Inclusive Method to Estimating Target Weight Range Goals. EDRD PRO.